Oncologists Charge 9 to 51% More for Physician-Administered Drugs
Their unique revenue structure and narrow network exclusion may be prompting oncologists to charge significantly more for common physician-administered drugs, a study showed.

Source: Thinkstock
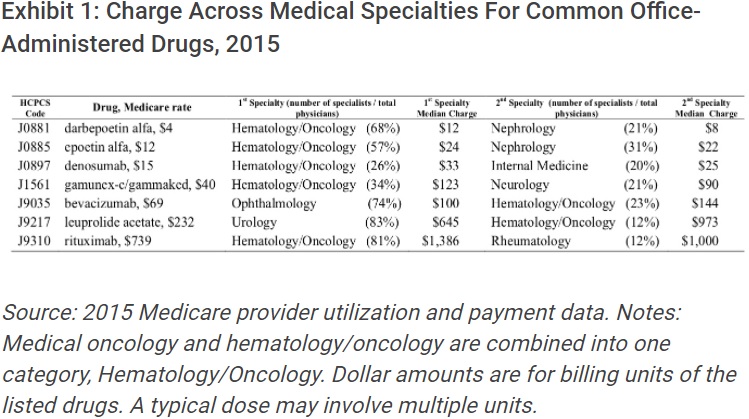
- Median charges for physician-administered drugs covered under Medicare Part B were 9 to 51 percent higher at the oncologist than other specialty offices, researchers from Memorial Sloan Kettering Cancer Center and Johns Hopkins University recently reported.
The results, published in a Health Affairs blogpost, showed that oncologists charged more for seven common physician-administered drugs with both oncology and non-oncology indications.
For example, the studied prescription drugs included darbepoetin alfa, which is used to treat anemia brought on by chemotherapy. Nephrologists also administer the darbepoetin alfa to treat anemia caused by kidney failure. Denosumab is also used to treat osteoporosis, as well as bone cancer.
While the seven physician-administered drugs were commonly used across several specialties, oncologists charged significantly more, which impacted uninsured or privately insured out-of-network patients.
The largest gap between what specialists charged was $328 for leuprolide acetate, a prescription drug that treats prostate cancer, endometriosis, and uterine fibroids. The median charge was $973 among oncologists and $645 among urologists.
Researchers observed the smallest gap for epoetin alfa, which is used to treat anemia. The median charge was $24 among oncologists and $22 among nephrologists.
Source: Health Affairs
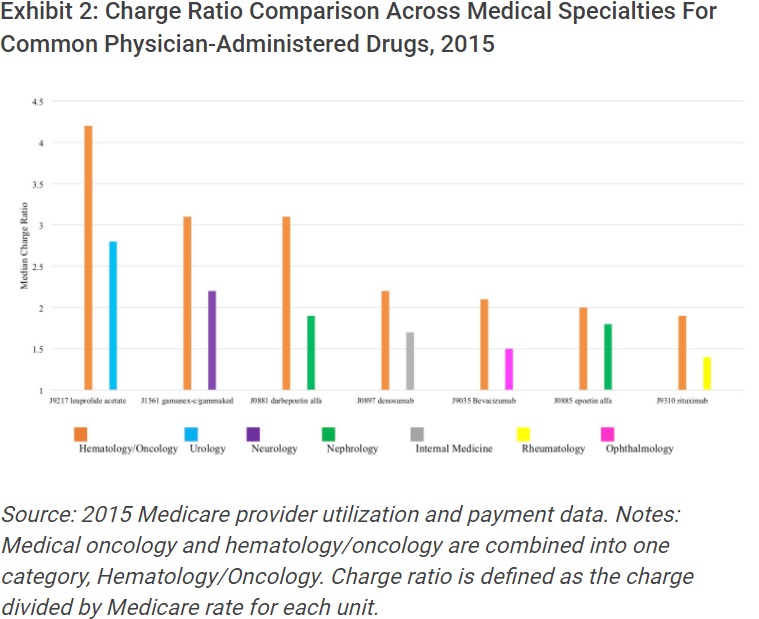
Oncologists also reported significantly higher median charge ratios, or the charge set by specialists divided by the Medicare reimbursement rate.
Medicare reimburses physician-administered drugs under Part B. The rate is the average sales prices plus 6 percent, which aims to cover the costs of storage, preparation, and safety monitoring of the prescription drug.
The Medicare reimbursement rate is independent of the charges set by specialists and the rate is the same for all specialists for the same drugs, researchers added.
The median charge ratio for all seven of the commonly used prescription drugs was higher among oncologists than other specialists. The median charge ratio for oncologists ranged from 1.9 to 4.2, while the median charge ratio for all other specialists ranged from 1.4 to 2.8.
Source: Health Affairs
Oncologists may be charging more for physician-administered drugs to maximize their revenue, researchers explained. Cancer care providers operate under a unique revenue structure because many oncology therapies cannot be self-administered by patients.
“Purchasing office-administered drugs is both a significant expense and revenue source for oncologists, a feature not shared by most non-oncologists,” researchers wrote. “As a result, oncologists and oncology group practices are probably motivated to focus on generating profit through office-administered drugs.”
Oncologists may also treat a greater proportion of out-of-network and uninsured patients, researchers hypothesized.
“The urgency associated with some types of cancer might make patients more inclined to seek care, thus leaving them with fewer opportunities to choose physicians and more likely to be treated by oncologists out of their insurance network,” they elaborated. “The growing popularity of narrow-network health plans, which limit patient access to providers, has only intensified this problem.”
Narrow insurance networks are an issue for cancer patients, according to a recent study from the Perelman School of Medicine. The analysis showed that oncologists affiliated with the National Comprehensive Cancer Network (NCCN) and National Cancer Institute (NCI)-Designated Cancer Centers were less likely to be included as in-network providers in narrow insurance networks despite NCCN and NCI having a reputation for high-quality care.
Privately insured patients who seek cancer care outside of their network are subject to the charges set by oncologists, meaning these patients are paying more for physician-administered drugs by not seeing an oncologist in their network. Although some providers will offer discounts for these patients.
Oncologists should prioritize patient financial responsibility discussions in light of narrow insurance networks trends, researchers advised.
Patients join narrow networks for lower premiums even though they have limited access to providers.
While there are trade-offs associated with narrow insurance networks, inadequate health literacy among plan beneficiaries may prevent individuals from understanding the patient financial responsibility consequences of joining a narrow network.
Only 12 percent of adults have proficient health literacy, the National Assessment of Adult Literacy reported. In other words, nearly nine out of ten adults do not have sufficient knowledge about their coverage or healthcare options.
Therefore, oncologists should improve healthcare price transparency and discuss patient financial responsibility to ensure cancer patients adhere to their treatment plans and medications.
“A potentially effective measure would be to make the charge of office-administered drugs transparent to out-of-network and uninsured patients, helping them comprehend their financial responsibilities,” researchers suggested. “Oncologists who apply generous discounts could make this known immediately to the patient, or more conveniently, reduce their charges of office-administered drugs.”